 It’s November, which means it’s Diabetes Awareness Month, and on the 14th it’s also World Diabetes Day (and more importantly, my Diabeteversary). So we thought, what better than to produce an article that the pancreatically-challenged among us can point our insulin-abundant friends to help explain our special club to them. This blog talks about diabetes from the point of view of Type 1 diabetes as that’s what our experience is of.
It’s November, which means it’s Diabetes Awareness Month, and on the 14th it’s also World Diabetes Day (and more importantly, my Diabeteversary). So we thought, what better than to produce an article that the pancreatically-challenged among us can point our insulin-abundant friends to help explain our special club to them. This blog talks about diabetes from the point of view of Type 1 diabetes as that’s what our experience is of.
What is diabetes?
When we eat carbohydrates (like pasta, rice, potatoes, sugary things) they get broken down into glucose in the intestine, and then absorbed into the blood stream. This is the same whether you have diabetes or not. The next stage is where things differ:
If you don’t have diabetes
The glucose in your blood tells your pancreas to produce insulin. The insulin acts like a key that unlocks your cells to allow the glucose inside to be used to make energy. The pancreas usually makes a small amount of insulin all the time, but makes more after meals when the blood glucose level rises due to taking on food.
If you have diabetes
The cells in the pancreas that produce insulin don’t work anymore. This means that when glucose goes into the blood, it can’t get into cells. Because your cells can’t get the glucose to make energy, they tell your body it needs more sugar, and so it starts to break down fat to make sugar. This causes blood glucose to rise more, and this cycle causes the blood to become acidic – making the person very unwell.
Type 1 vs Type 2
You might have heard of different types of diabetes, and though it’s more complicated than this, here’s a handy guide to the difference.
Type 1
Type 1 diabetes is a condition where the body’s immune system destroys the cells in the pancreas that produce insulin. People with Type 1 diabetes always need to take insulin as they do not produce any of their own.
Type 1 usually presents earlier in life – in childhood through to early adulthood – although it can occur at any time. In older adults it can be less clear at first which type of diabetes they have – but a test can be done for something called c-peptide to find out.
Type 2
Type 2 diabetes is a slightly more complex condition. Initially, people with type 2 diabetes are producing their own insulin, however their body becomes less sensitive to it. This can progress so that they do not produce any insulin anymore, but this is not because their immune system has destroyed the cells. Type 2 diabetes can be treated in a number of ways, from diet and lifestyle changes initially, through various tablets, and finally using insulin.
Why do people get Type 1 Diabetes?
Short answer: we don’t really know. At the moment the best theory is that people have a gene that makes them more likely to develop diabetes, however that it doesn’t develop until something triggers it – this might be a virus, an environmental trigger or something else entirely we haven’t thought of yet.
Definitely not reasons people get Type 1 Diabetes: eating too many sweets, being too fat.
What are the symptoms of diabetes?
 Before people are diagnosed with diabetes, their symptoms normally fit into the pattern shown by the 4 T’s Campaign run by DiabetesUK.
Before people are diagnosed with diabetes, their symptoms normally fit into the pattern shown by the 4 T’s Campaign run by DiabetesUK.
One of the first things people will probably notice is feeling tired and run down. The glucose in blood cannot get into cells, and so people feel like they have no energy.
They might also notice their clothes becoming looser as they lose weight. As the glucose in blood cannot be used by cells, fat is burned, causing weight loss.
Toilet and Thirsty are closely connected. I thought I was peeing a lot because I was drinking a lot, but actually it is the other way around. The kidneys try to get rid of the excess sugar by making you pee more, which makes you thirsty.
Insulin Therapy
People with Type 1 diabetes ALWAYS need insulin, however this can be given in a number of different ways, however there are two main regimes in use today:
Multiple Daily Injections
This is also known as ‘basal-bolus’. People using this approach have two different types of insulin.
They have a long-acting insulin – this might be called Lantus or Levemir. These insulins usually last 18-24hrs in the body, that they take once or twice a day. This imitates the small amounts of insulin that the pancreas normally makes all the time.
The other type of insulin is a short-acting insulin – for example Novorapid or Humalog. These insulins get to work very quickly (within around 15-30 minutes) and finish acting after a few hours. These insulins are taken at mealtimes, to imitate the action of the pancreas in response to food.
Between the two types of insulin, people on MDI might expect to be injecting between 4 and 8 times a day, depending on how many meals and snacks they eat.
Insulin Pumps
An insulin pump is basically like one half of an artificial pancreas. It is able to do the basal job of the pancreas, releasing small amounts of short acting insulin continuously. The user is then able to get it to do the food response job too, but only by taking into account their current blood sugar level and the carbohydrate content of food.
The pump is connected to a small flexible tube that sits in the skin for a few days at a time.
SUB-FAQ: Insulin Pumps
- Does the cannula hurt?
Sometimes. Mostly you don’t notice they’re there, but you’re sticking something into your skin, so sometimes it gets irritated and can be a bit painful. - How often do you change it?
It varies a bit from pump to pump, but usually cannulas need changing every two to three days. This usually only takes a few minutes to do. - Do you only get a pump if you are good/bad at controlling your diabetes?
No. There are a range of reasons you can get a pump, depending on what your consultant thinks. Some people will get them because they are having difficulty with their control (this is NOT the same as being bad at it), others because they have specific lifestyle factors that make a pump more helpful.
What is an acceptable blood glucose level?
The official targets are:
- on waking: 5–7mmol/l
- before meals at other times of the day: 4–7mmol/l
- 90 minutes after meals: 5–9mmol/l
However, these are the ‘ideal’ – different people might have different targets. Someone who has been having bad hypos, or has no hypo awareness might let their levels run a little higher, for example.
More socially though, an acceptable blood glucose is whatever the person with diabetes says it is. We will have a low tolerance for lecturing from others.
Should you be eating that piece of cake?
My sassy answer to this question is ‘should you?!’
This might seem a bit sarcastic, but there’s truth in it. People with diabetes are just as entitled to make ‘naughty’ food choices as anyone else. There are no banned foods for people with diabetes.
Asking this question is pretty insensitive, to be perfectly honest. If I am ordering a sticky toffee pudding in a restaurant, it’s a guilty pleasure. Asking me if I should be having it takes the joy out of it.
If you find yourself wanting to ask this question, don’t.
Diabetic Diet
There is no such thing. Some of us might choose to do certain things we’ve found keep our blood sugar levels more stable – for example if we eat a low carb diet, then some people find this helps them with their control. Others don’t. It’s all individual. It’s about finding what works for the individual – both in terms of control and also in terms of allowing them to live the life they want.
Hypos
When blood glucose falls below 4.0mmol/l this is known as a hypo (short for hypoglycaemia, which is fancy medicalese for not enough sugar in the blood). They are caused by having too much insulin for the amount of glucose in the body. This can be due to a miscalculation in dose, or due to increased activity.
Hypos are a spectrum, they range from being a minor inconvenience through making you feel quite unwell to – at the extreme – being a medical emergency that can cause coma and death.
Symptoms
Someone having a hypo can quite suddenly start to feel unwell, and there are a variety of different symptoms that can differ from person to person.
- shakiness
- sweating
- hunger
- becoming an arsehole out of nowhere
- headaches
How you can help
First up is the REALLY important way you can help. If we pass out DO NOT DO NOT DO NOT try to feed us anything. We will choke, and this will make things many times worse. If we pass out CALL AN AMBULANCE.
If we suddenly start being a dick, and it’s because of our blood sugar going low, know that we don’t mean it, we love you and we’re sorry.
If we go pale and quiet, offer us something sugary to eat or drink.
Sub-FAQ: Hypo treatments
To treat hypoglycaemia, we need fast acting sugar.
Examples of things that are good for hypos:
- Fruit Juice
- Coke
- Lucozade
- Jelly Babies
- Dextrose tablets
- Sweets
Things that are not good for hypos (they are all too slow to be useful):
- Chocolate
- Crisps
- Bread
- Milk
Hyperglycaemia
Hyperglycaemia is less of an emergency than hypos – high blood glucose causes problems over the longer term more than the short term, although there is an exception to this.
You might be able to spot if we have high blood sugar from the following symptoms:
- We go to pee A LOT
- We’re really thirsty
- We complain about headaches
- We become tired
- We become mega grumps.
In these cases, mostly we just need a nudge to test and take a correction dose of insulin.
Diabetic Ketoacidosis
Sometimes, if we’re unwell or we miss our insulin we can get very high blood glucose, and because our cells aren’t able to use it to make energy, we produce chemicals called ‘ketones’. These make the blood acidic and make us very unwell, very quickly.
DKA is a life-threatening emergency.
If this happens, the most important thing is that we get to A&E where we can be treated.
It’s Complicated
Diabetes, over time, can cause a range of complications in lots of different parts of the body. Good blood glucose control can make this less likely. These are things that all people with diabetes need to think about.
The main groups of complications can be split into those that affect bigger blood vessels and those that affect smaller ones. The way that each of these is caused is basically the same – high blood sugar over time causes sugar to stick to the lining of blood vessels causing it to become thicker and weaker.
Big Blood Vessels
Heart Attack/Stroke
Thickened vessels can lead to conditions like heart attack or stroke, particularly if the person also has had high cholesterol, or has smoked.
Peripheral Vascular Disease
In the same way, if vessels become narrow in the legs then the blood supply to the legs is reduced. This can be painful and can reduce the ability to do things.
High Blood Pressure
Blood forced through narrower vessels is at a higher pressure, and this is bad as it increases the stress on the vessels.
Small Blood Vessels
Nephropathy (Kidneys)
Over time, with high blood sugars, the kidneys can become leaky and scrred. This can mean that they become less good at filtering the blood, and less effective at removing toxins from the blood.
Neuropathy (Nerves)
Nerves are surrounded by tiny blood vessels that supply them. If these vessels are affected then the nerves can start to malfunction, either producing painful symptoms or a loss of sensation altogether. This is one of the reasons that diabetic people need to be careful about their feet as if they have neuropathy then they might damage their foot without noticing.
Retinopathy (Eyes)
The tiny vessels at the back of the eye can get blocked. This can cause a progressive loss of vision – sometimes resulting in blindness, and in some cases can causes bleeds into the eye.
What’s that?
Us diabetics have a bewildering array of kit that often intrigues the pancreatically-abled. Here’s a run down of the thing your mate is playing with.
Blood Glucose Meter
 These come in all types of shapes and sizes. But they all come down to a meter, test strips (which are single use) and a lancet (to get the blood out). The strip goes into the meter, the blood onto the strip and a few seconds later we have a reading. Some are more complex than this, recording readings to be shown on a graph to see trends, but basically they all do the same job.
These come in all types of shapes and sizes. But they all come down to a meter, test strips (which are single use) and a lancet (to get the blood out). The strip goes into the meter, the blood onto the strip and a few seconds later we have a reading. Some are more complex than this, recording readings to be shown on a graph to see trends, but basically they all do the same job.
Does it hurt to prick your finger?
Sometimes.
Insulin Pen
 Rather than faffing around with vials of insulin and syringes, those of us who inject our insulin usually use pens. These are either disposable or refillable, with an easy way to dial up a dose and easy to change needles.
Rather than faffing around with vials of insulin and syringes, those of us who inject our insulin usually use pens. These are either disposable or refillable, with an easy way to dial up a dose and easy to change needles.
Does it hurt to inject?
Sometimes.
Insulin Pump
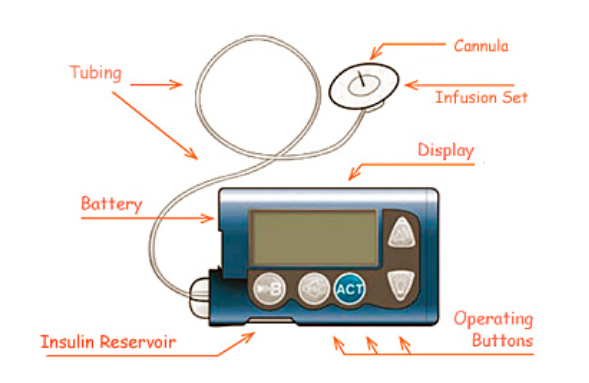 The lucky among us might have an insulin pump. These vary a bit between different manufacturers, but mainly they all have a cannula (to enable the insulin to get into the body), a reservoir to hold the insulin, and a display and buttons to allow the user to control the pump.
The lucky among us might have an insulin pump. These vary a bit between different manufacturers, but mainly they all have a cannula (to enable the insulin to get into the body), a reservoir to hold the insulin, and a display and buttons to allow the user to control the pump.
If you are curious about our pumps, do ask us, we’re often very happy to show off about them.
Ketostix
These are basically test strips that we wee on. It can tell us how many ketones are in the urine, and this can be a warning of DKA.
Continuous Glucose Monitor
 The very luckiest among us have the fanciest kit. A continuous glucose monitor (CGM) has a small sensor that sits int the skin and measure the glucose level constantly, sending signals to a handset. This gives users a realtime picture of what is happening with their glucose level
The very luckiest among us have the fanciest kit. A continuous glucose monitor (CGM) has a small sensor that sits int the skin and measure the glucose level constantly, sending signals to a handset. This gives users a realtime picture of what is happening with their glucose level
